Introduction
Platinum-based compounds play an integral role in chemotherapy treatments for various forms of cancer. One such platinum compound, Cisplatin, has received widespread acclaim as an effective cancer fighter.However, it is essential to realize that cisplatin is not the only platinum-based compound available; transplatin, another closely related compound with similar characteristics but unique distinctions, offers additional alternatives.
Examining the distinctions between cisplatin and transplatin is critical for understanding their unique properties, potential applications, and impactful role in treating cancer. This content outline aims to explore the distinctions between cisplatin and transplatin, exploring their chemical structures, formation, stability, biological activities, medical applications, resistance patterns, side effects, and current research.
By understanding their similarities and dissimilarities, researchers and medical professionals can make more informed decisions when selecting these compounds for cancer therapy and potentially introduce novel treatment approaches.
Definition of Cisplatin
Cisplatin is a Chemotherapy drug from the class of platinum-Containing compounds and is widely used to treat Various cancers such as testicular, ovarian, bladder, lung and head and neck cancers. Cisplatin has proven its anticancer capabilities through numerous chemotherapy regimens.
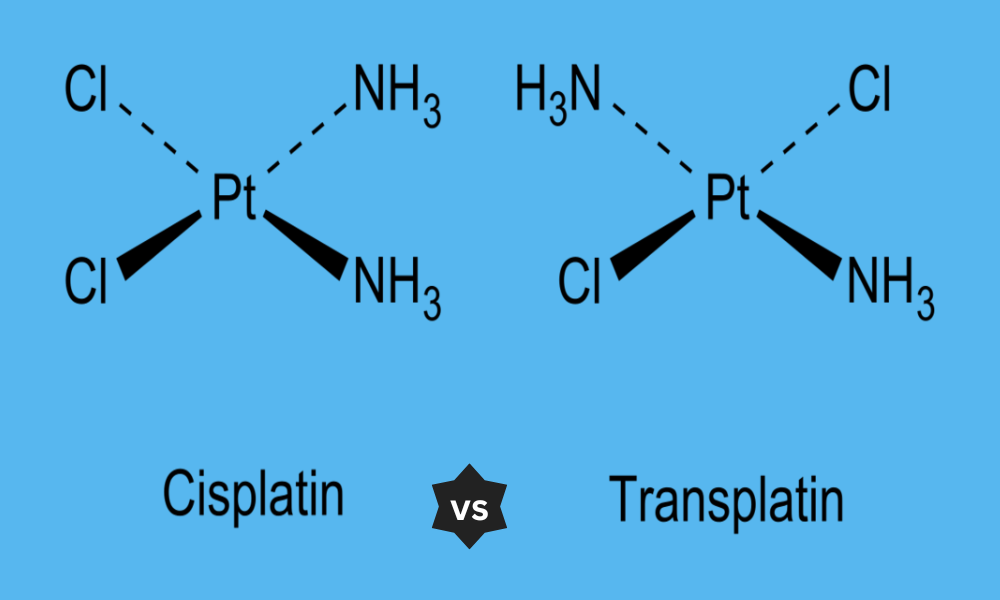
Chemically speaking, cisplatin is a coordination compound consisting of one central platinum atom surrounded by two chloride ions and two amine groups. The name “cisplatin” refers to how both chloride ions occupy opposite sides of the platinum atom; hence its name as well.
Cisplatin’s anticancer effects are achieved by forging covalent bonds with cancer cell DNA molecules, leading to cross-linking and DNA damage that impair their ability to divide and replicate, ultimately leading to cell death.
Cisplatin can be an Effective cancer Chemotherapeutic agent; however, its side Effects include kidney damage, nausea and vomiting as well as Hearing loss and peripheral Neuropathy. These adverse reactions occur due to its nonselective toxicological action against both cancer cells as well as healthy cells within the body.
Cisplatin has been extensively researched and utilized clinically since its discovery in the 1960s. Today it remains one of the cornerstone drugs for cancer therapy; often used intravenously alongside other chemotherapy medications to increase effectiveness while minimizing resistance development.
Definition of Transplatin
Transplatin is a chemical compound closely related to cisplatin that belongs to the same family of platinum-containing compounds. Both substances share similar chemical structures and properties; the two differ only in their arrangement of their ligands. Transplatin is similar to cisplatin in that it contains a central platinum atom surrounded by ligands; however, their arrangement differs as transplatin’s ligands are located on opposite sides of its platinum atom.
Transplatin has been researched for its potential therapeutic uses in treating anticancer. Like cisplatin, transplatin forms covalent bonds with DNA molecules to cause damage and limit cancer cell proliferation; however, transplatin has different biological activity and properties than its cisplatin counterpart. Transplatin is not as well-known or frequently utilized clinically; however, transplatin has received less research attention and consideration. Its potential as an anticancer agent and its efficacy, toxicity and resistance patterns is still being evaluated.
Transplatin is not widely utilized for cancer treatments in clinical settings; cisplatin remains the preferred platinum-based chemotherapy drug. Research and clinical applications related to platinum-based chemotherapy have focused on cisplatin and its derivatives.Further studies and research are necessary in order to fully comprehend and appreciate transplatin’s therapeutic potential and limitations, and identify its specific role in cancer therapy.
Comparison Table of Cisplatin and Transplatin
Sure! Here’s a comparison table highlighting the key differences between cisplatin and transplatin:
| Aspect | Cisplatin | Transplatin |
|---|---|---|
| Chemical Structure | Square planar coordination complex | Octahedral coordination complex |
| Ligand Arrangement | Cis configuration (ligands on the same side) | Trans configuration (ligands on opposite sides) |
| Formation | Synthesized from platinum precursor compounds | Synthesized from platinum precursor compounds |
| Stability | Relatively stable | Relatively less stable |
| Biological Activity | Forms covalent bonds with DNA, causing DNA damage and inhibiting cancer cell growth | Forms covalent bonds with DNA, but exhibits different biological activity compared to cisplatin |
| Efficacy and Toxicity | High efficacy against certain types of cancer, but also associated with significant side effects such as kidney damage, nausea, and hearing loss | Comparative efficacy and toxicity profile is still being explored, and its use in clinical settings is limited |
| Medical Applications | Wide range of cancer types, including testicular, ovarian, bladder, lung, and head and neck cancers | Limited clinical applications, currently under investigation for potential therapeutic uses |
| Resistance Patterns | Development of resistance can occur over time | Resistance patterns and mechanisms are still being studied |
| Current Research | Extensive research and clinical use | Limited research, but ongoing exploration of its properties and potential applications |
It’s important to note that the information provided in the table is a general overview and may not encompass all aspects and nuances of cisplatin and transplatin. Further research and consultation with medical professionals are recommended for a comprehensive understanding of these compounds.
Importance of understanding the difference between the two compounds
Understanding the difference between cisplatin and transplatin is of critical importance for several reasons.
Treatment Optimization: Healthcare professionals can improve cancer patient treatment strategies by understanding the differences between cisplatin and transplatin, thanks to their respective biological activities, efficacy profiles and toxicities. Their various effects may affect treatment selection, dosing regimens or combinations therapies.
Personalized Medicine: Personalized medicine strives to tailor treatments specifically to each patient based on their unique characteristics. Understanding the differences between cisplatin and transplatin can aid in devising tailored plans taking into account factors like cancer types, genetic characteristics, drug sensitivities and more.
Minimizing Side Effects: Both cisplatin and transplatin can cause side effects, though their profiles may differ significantly. Being aware of this difference can help minimize their occurrence and severity by selecting an ideal medication based on each patient’s individual circumstances.
Resistance and Treatment Failure: Cancer cells often develop resistance to chemotherapy drugs, leading to treatment failure. By studying the differences between cisplatin and transplatin, researchers may discover strategies to overcome resistance mechanisms or identify alternative treatment options.
Advance Drug Development: Knowing the unique properties and mechanisms of action of cisplatin and transplatin can aid researchers in creating new platinum-based compounds with improved efficacy and reduced toxicity, potentially leading to the discovery of novel medicines that surpass any limitations associated with current therapies containing platinum.
Research and Clinical Trials: Knowledge of the differences between cisplatin and transplatin is vital when conducting studies or trials that assess their efficacy or safety, since accurate interpretation and comparison depend upon understanding each compound’s individual properties.
Understanding the differences between cisplatin and transplatin is integral for informed decision-making in treatment selection, individual patient care and drug development, research advancement and drug discovery efforts as well as optimizing cancer treatment strategies and thus ultimately improving patient outcomes.
Highlighting the key structural differences between cisplatin and transplatin
The key structural differences between cisplatin and transplatin can be summarized as follows:
Ligand Arrange: One of the key differences between cisplatin and transplatin is in their respective arrangements of their ligands around their central platinum atom. Cisplatin’s ligands are located on one side of its core; for transplatin on its opposite sides resulting in trans configuration.
Shape: Ligand arrangements significantly impact the overall shape of compounds. Cisplatin has a square planar form with all its ligands lying on one plane; transplatin forms an octahedral shape with all ligands located at corners of an imaginary octahedron containing its central platinum atom.
Steric Effects: Due to their differing ligand arrangements, cisplatin and transplatin each display different steric effects. With cisplatin, its bulkier arrangement could interfere with interactions with other molecules; while with transplatin’s more open structure from having its ligands on opposite sides.
Chirality: Cisplatin and transplatin differ significantly when it comes to their chirality. Cisplatin exists as two enantiomers (mirror-image isomers) that cannot be superimposed, while transplatin lacks stereocenters resulting in no chirality at all.
These structural differences between cisplatin and transplatin can alter their reactivity, binding affinity to biological molecules, and interactions with target cells – understanding these variances is vital to understanding any disparities in biological activities, pharmacokinetics or therapeutic potential between them.
Discussion on the stability of cisplatin and transplatin
Stability refers to the ability of cisplatin and transplatin compounds to maintain their chemical integrity under different environmental conditions without degrading into decomposable forms or decomposition, decomposition or degradation. Both contain platinum atoms; however, their stability varies due to different structural arrangements.
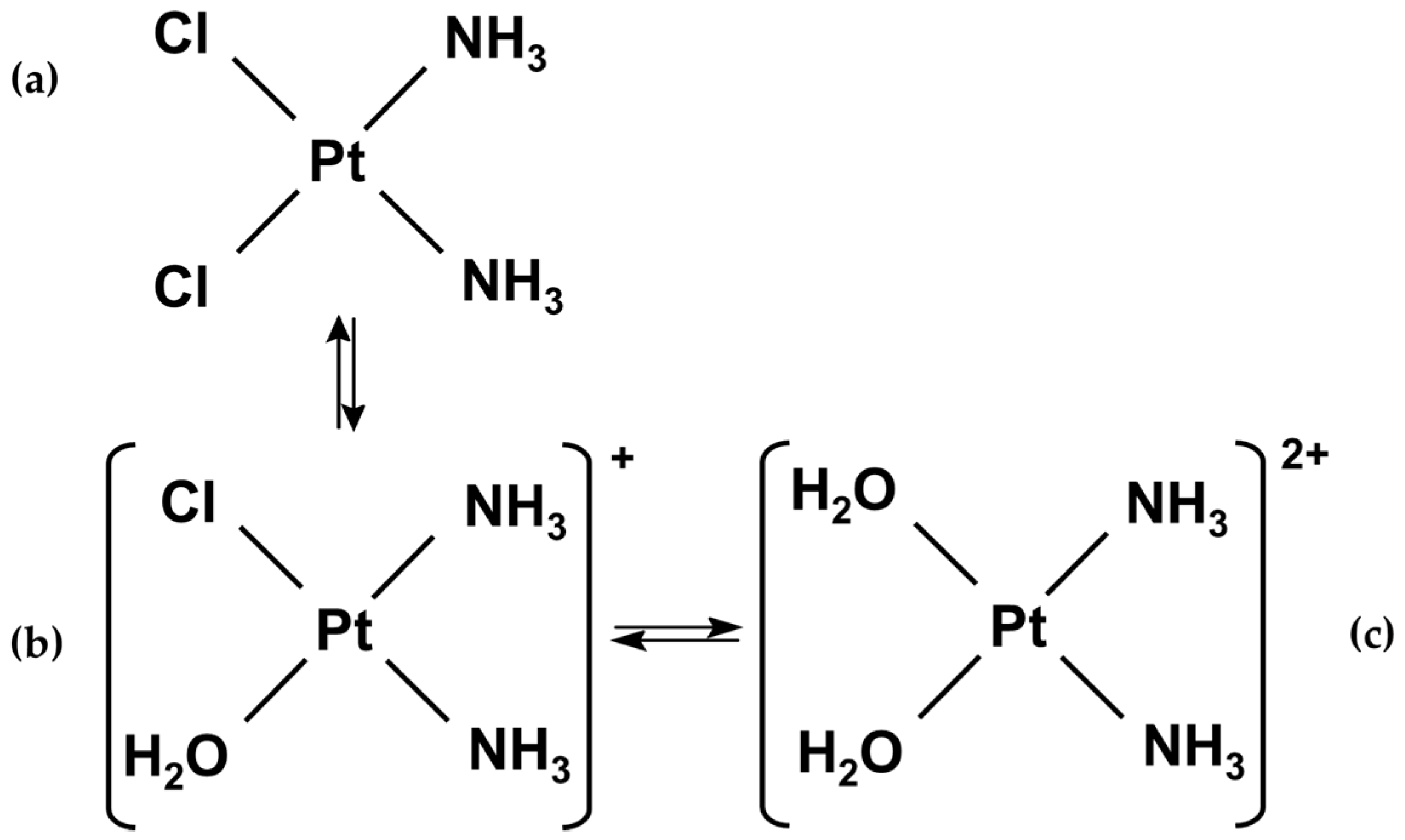
Cisplatin is widely acknowledged to exhibit high stability under physiological conditions. Its square planar configuration and strong platinum-chloride bonds help ensure resistance against degradation in the body, which allows cisplatin to reach target sites more quickly and exert anticancer effects effectively. However, hydrolysis reactions in aqueous solutions may result in aquated species that alter its biological activity and decrease its effectiveness.
Transplatin is often considered less stable than its cisplatin counterpart due to the trans configuration, in which ligands are located on opposite sides, creating structural flexibility which makes transplatin more susceptible to substitution or reaction with other molecules, potentially altering its pharmacokinetics, biological activity, and overall efficacy as an anticancer agent. Therefore, transplatin may require special handling and storage precautions in order to preserve its integrity for research or therapeutic applications.
Note that both cisplatin and transplatin can be affected by various factors, including pH, temperature, chemical species present and their environment of administration. Furthermore, stability can differ in various formulations or when combined with other agents in chemotherapy regimens.
Enhancing the stability of platinum-based compounds to increase therapeutic efficacy and decrease side effects is a priority for pharmaceutical researchers, and efforts to do so are underway. Strategies employed to improve their performance may include changing ligands or structures or encasing platinum complexes within nanoparticles or drug delivery systems as ways of increasing stability and optimizing performance of these compounds.
Understanding and assessing the stability of cisplatin and transplatin is vital for their effective use in cancer therapy, as this factor affects bioavailability, pharmacokinetics, and interactions with cancer cells directly.
Examination of the mechanisms of action for both compounds
Cisplatin and transplatin both work by interfering with DNA to cause damage, leading to cell inhibition and ultimately stopping cancer cell growth. Their interactions can differ in terms of specifics and results depending on which compound you take; details and outcomes may also vary between compounds.
Cisplatin’s Covalent DNA Binding Mechanism: When administered, cisplatin enters cancer cell nuclei where it undergoes aquation to form positively charged platinum aqua complexes which then adhere covalently to DNA molecules by binding with purine bases (especially guanine) on DNA strands, creating covalent bonds between these complexes and DNA molecules, often creating an adduct with purine bases like guanine that form on those same strands.
Cross-Linking DNA: When covalently bound with DNA, cisplatin causes both intrastrand and interstrand cross-links to form. Intrastrand links occur when platinum atoms bind to adjacent purine bases on one strand while interstrand cross-links form when platinum atoms simultaneously bind with purine bases on different strands simultaneously.
DNA Cross-Links and Their Effects: When DNA replication or transcription processes become impaired by cross-links, DNA damage occurs resulting in disruption of normal cellular functions, prompting various responses in cells such as activating DNA repair mechanisms, cell cycle arrest or initiating apoptosis (programmed cell death). This ultimately triggers various responses such as activating DNA repair mechanisms or initiating apoptosis (programmed cell death).
Indirect Effects: Cisplatin can also increase production of reactive oxygen species (ROS) and alter cellular redox balance, leading to further DNA damage and oxidative stress. The mechanisms of action for transplatin are similar to cisplatin.
Due to structural dissimilarities there may be slight variations. Both drugs interact with DNA by covalent binding, leading to damage of cancerous cells; however the details and efficacy of transplatin’s interactions may differ slightly from that seen with cisplatin – further research must be completed to fully elucidate transplatin’s mechanisms of action.
Note that while cisplatin and transplatin primarily target DNA, they can have additional effects on other cellular components and signaling pathways to increase anticancer activities. Furthermore, their precise mechanisms of action are complex, possibly including direct DNA interactions as well as indirect effects or cellular responses.
Understanding the mechanisms of action behind cisplatin and transplatin is vital to optimizing their therapeutic use, developing strategies to counter resistance, and identifying potential targets for combination therapies. Our ongoing research endeavors seek to gain more insight into this subject as we investigate further the full potential of platinum-based compounds for cancer therapy treatment.
Analysis of the development of resistance to cisplatin and transplatin
Resistance to cisplatin and transplatin can be an enormous barrier in cancer therapy. Cancer cells may acquire various methods to evade their cytotoxic effects, leading to treatment failure and disease progression.
Resistant mechanisms include genetic, cellular, tumor microenvironment-related factors as well as factors specific to each compound such as genetic mutation. Cisplatin resistance has been extensively researched whereas research on transplatin resistance remains limited but some resistance mechanisms may share traits with both compounds – Here are a few key factors associated with both compounds:
Decreased Accumulation: Resistance can arise through reduced uptake or increased efflux of platinum-based compounds by cancer cells, alterations to membrane transporters such as CTR1, ABCB1, ABCC2 transporters or other transport proteins can reduce intracellular accumulation of cisplatin or transplatin thus decreasing its cytotoxic effects and rendering treatment ineffective.
Increased DNA Repair Capacity in Cancer Cells: One of the main resistance mechanisms against chemotherapy drugs is increased DNA repair capacity within cancer cells. By activating DNA repair pathways such as nucleotide excision repair (NER), mismatch repair (MMR), and homologous recombination (HR), cancer cells can efficiently repair DNA damage caused by cisplatin and transplatin, decreasing their cytotoxic effects.
Changed Platinum-Binding Targets: Resistance can develop due to changes in the molecular targets of cisplatin and transplatin. Cancer cells may alter the structure or expression of DNA-binding proteins involved in platinum-DNA interactions such as high mobility group proteins (HMGB1) or nucleolin, leading to altered platinum-DNA interactions that reduce their effectiveness as chemotherapy drugs. Such changes could reduce cytotoxic effects as a result.
Changes to Cellular Signaling Pathways: Dysregulation of signaling pathways involved with cell survival, apoptosis and cell cycle regulation may contribute to platinum resistance. Activation of survival pathways like PI3K/Akt and MAPK/ERK may promote cell survival while conferring resistance against the effects of cisplatin and transplatin-induced apoptosis.
Tumor Microenvironment Factors: The tumor microenvironment – including factors like hypoxia and stromal interactions – can have a major influence on platinum resistance. Hypoxic conditions in tumors may decrease cancer cells’ susceptibility to platinum compounds; furthermore, interactions between cancer cells and components of their microenvironment, like cancer-associated fibroblasts (CAFs) or immune cells can play a key role in creating resistance via paracrine signaling or immunosuppression.
Resistance to cisplatin and transplatin is often multifactorial, involving different mechanisms outlined above. Furthermore, these resistance mechanisms may vary across cancer types or even individuals undergoing therapy; understanding their origin is therefore key for devising strategies to overcome or prevent resistance, including combination therapies targeting specific pathways or biomarkers to guide treatment decisions.
Further research is necessary to understand the specific mechanisms of transplatin resistance, as well as any differences compared to cisplatin. By uncovering these resistance mechanisms, researchers can create innovative strategies to increase effectiveness of platinum-based therapies and thus improve patient outcomes.
Comparison of the side effects associated with cisplatin and transplatin
Cisplatin and transplatin, as platinum-based compounds, may both cause side effects. While some symptoms may be similar across both treatments, their frequency and severity can differ – as can individual patient responses; side effects are dependent on factors like dosage duration and overall patient health status.
Here is a Comparison between some Common side effects Associated with both Treatments:
Kidney Toxicity: Both cisplatin and Transplatin can cause kidney damage, Commonly referred to as Nephrotoxicity, which can result in Impaired kidney function, electrolyte Imbalances and reduced urine output. Careful Monitoring and proper hydration measures should be Implemented while using either Compound.
Nausea and Vomiting: Cisplatin is widely known for its strong emetogenic potential, often leading to severe nausea and vomiting in users. Transplatin may produce similar side effects; the severity may differ between individuals.
Ototoxicity: Cisplatin and transplatin can both cause inner ear damage that leads to hearing loss and/or tinnitus, with risk and severity varying among patients; it’s often more prevalent after receiving treatment with cisplatin than transplatin.
Peripheral Neuropathy: Cisplatin treatments may lead to peripheral neuropathy, an effect which manifests itself by numbness, tingling or pain in the hands and feet. Although transplatin treatment has less been studied as far as its frequency or severity are concerned, peripheral neuropathy could still be an unwanted side effect of treatment.
Hematological Effects: Cisplatin and transplatin can have serious hematological side effects. Both medications may reduce white blood cells, red blood cells, and platelets resulting in greater susceptibility to infections, anemia, and bleeding complications.
Gastrointestinal Effects: Cisplatin and transplatin treatments may lead to gastrointestinal side effects such as diarrhea or constipation in some individuals; their frequency and severity depend on individual circumstances.
Allergic Reactions: Although rare, both cisplatin and Transplatin may cause allergic Reactions ranging from mild skin rashes to more serious Hypersensitivity reactions that require medical Intervention immediately if any signs of an allergic reaction surface. If any such signs arise, Medical attention should be sought Immediately.
Before Initiating treatment with either Cisplatin or transplatin, it is vitally Important to discuss any Potential side effects with a Healthcare provider. Their team will closely manage any adverse reactions during this process in order to maintain patient wellbeing and quality of life while on chemotherapy treatment.
Strategies such as supportive care, dose adjustments or combination therapies may be employed in order to mitigate side effects and optimize treatment results.
Conclusion
Understanding the differences between cisplatin and transplatin is of utmost importance for researchers, medical professionals and cancer patients in treating cancer. While both substances share similarities as platinum-based drugs, they possess distinct chemical structures, mechanisms of action, side effects and potential applications.